Most medical equipment companies don't regularly top "most innovative" lists.
But D-Rev isn't your typical medical device maker. The San Francisco-based non-profit wants to help the world's poorest individuals, who subsist on less than a few dollars per day. Its products include an $80 prosthetic knee and a phototherapy device to treat infants with jaundice.
[Skip to the bottom of the article to watch a TED talk on the $80 ReMotion knee.]
What's unique about D-Rev is its approach to research. The company sends its small team of designers into the field -- whether it's a rural village in India or a remote hospital in Uganda -- to conduct interviews with patients, doctors and nurses.
During a recent conversation with a doctor based in rural India, D-Rev employees learned that many babies were dying of jaundice. The treatment devices were too expensive to maintain. The team brainstormed low-cost solutions and came up with Brilliance, a photo-therapy lamp that sells for $400, a fraction of the cost of its mainstream competitors.
Sponsored
KQED sat down with Krista Donaldson, the company's chief executive, to discuss the ongoing challenges of running a medical non-profit and the opportunities for the future. Donaldson shared that D-Rev is considering a move into the U.S. market to help those in need closer to home.
This interview has been condensed and edited for brevity.
In the past few years, D-Rev seems to have exploded in the media. When did the company get its start?
It was started in 2008 as a skunk-works of technology for the developing world. I was brought in because a lot of the products were in stages of prototyping and weren't reaching users. I cancelled most of the projects and focused our attention on people who are living on less than $4 a day. Our core mission is to close the gap in quality health care by focusing on delivery and design.
What was the first product that you released as CEO?
It was the Brilliance photo-therapy device. We got the idea after a doctor from India approached us at a conference. He said that the global health community, which is very Western-driven, is focused on the 'big ticket items' like preterm births and asphyxia [a potentially-fatal condition caused by a lack of oxygen in the blood.] But he told us that at his hospital, many babies were dying of jaundice. We estimate that 6 million babies with severe jaundice are not receiving adequate treatment.
My colleague got intrigued about developing a device that would shine an intense, blue light onto the baby's skin as a safe and effective therapy. We had heard that a hospital in Uganda was putting babies in the sun to get treated. This isn't safe, but the doctor did that because it was his only option.
[Watch the video below to learn more about D-Rev's solution.]
Many medical device companies will donate surplus equipment to developing nations. So why would health providers buy a product from D-Rev?
The medical device industry is far behind in terms of design. The approach they often take when thinking about low-income people is to donate the stuff that isn't being used in the West. There are all sorts of problems with that, whether it's different electronic frequencies, plugs and outlets, fluctuating temperature standards, or broader cultural issues.
How about low-income people in the U.S. who struggle to access cost-effective therapies? Are you planning to build devices for the domestic market?
Yes. We are in the early exploration phases of looking into low-income amputees in the United States. If we do something, it'll be a version of our prosthetic knee. The problem is that devices are so expensive here that many low-income people we've spoken to say they are ordering stuff from China on eBay. We'll have more information about our next steps later in the year.
What's your design process like for developing a new medical device?
We start with a problem identified by a user, oftentimes a doctor at a rural clinic. One example might be a lack of high-quality, affordable prosthetic knees. We would ask questions to potential users like: 'Would you want a prosthetic that will help with your gait? Are you looking for a device that will help you to return to work?'
When we were doing the prototype of Comet, an offshoot of our Brilliance phototherapy device, we drove around India and stopped at 20 different hospitals and clinics of all sizes to talk to the doctors. At this stage, we had four rough prototypes. Once you get more information, you can show the prototypes and get feedback. We also take into account cultural norms.
Once the product has been designed, we deal with things like regulation and intellectual property. Regulation is different in every country -- some have no requirements at all.
Donaldson interviewing an amputee victim (D-Rev)
Travel to rural parts of the world is expensive. Is it an ongoing challenge to raise funding?
We are raising money constantly. It is a challenge because we are more like a medical device startup than a typical philanthropic organization. We don't fit neatly into a bucket within the global health community, like USAID [the government agency responsible for administering foreign aid.] Their typical idea of global health innovation tends to be very labs-based.
But we have had a lot of success with foundations and individuals. Some companies help us out too, like Autodesk, which provides free software.
One big frustration I have is that big funders want to see data about improving mortality rates. They are less inclined to fund devices that prevent brain damage, rather than just save lives. We have to make sure that people can live healthy lives.
Aside from funding, what are some of the biggest hurdles that the company faces?
A lot of our users have low-trust in medical devices in general, in large part due to poor quality of some of the less expensive ones. Doctors often say to us: 'Why is your product so cheap? What's wrong with it?'
Another lesson learned is that in many low-income countries the government will purchase large batches of medical devices for state hospitals. They put out a tender with specifications that companies need to meet. I expected there to be less corruption in that process. But I'm hoping that things will improve over time with greater transparency.
What is the core demographic for D-Rev's devices?
We don't have any good data yet. But we are starting to do some preliminary research on gender. We have learned that boy babies are brought in for jaundice far more frequently than the girls -- it's about two to one. But boys and girl babies are equally likely to suffer from jaundice.
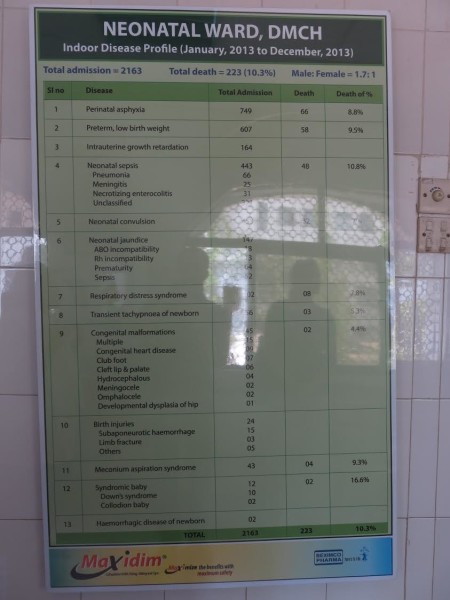
A snap of some data compiled by a hospital in Bangladesh (D-Rev)
We had heard that stat anecdotally for a long time, but it wasn't really apparent until we were in a hospital in Bangladesh last year and spotted a board filled with the data. It clearly showed more male babies.
We're spotting similar trends with our research into prosthetics. Female amputees will come into the clinic less frequently than men. We think it may be related to social stigma.
What have been a few of your high and low points at D-Rev?
My background is that I worked in Kenya for a number of years designing water pumps for farmers. I don't have as much experience in health.
The first time I was in a hospital in India, it was very upsetting. I was a new mother myself. There were these teeny tiny babies that could fit in the palm of your hand. And they were under these photo-therapy devices that I could tell were ineffective in one glance.
It was a low point, because I couldn't help but step back and think, 'these are lives that could be damaged permanently, but it's all so easily fixed.' My goal now is for everyone on our team to undertake at least one trip like this a year.
A high-point involves meetings with our users. I met a young woman called Poornima, who lost her leg in a car accident. She lost her brother in that accident. Poornima had wanted to be an engineer. Now, she wears one of our prosthetic knees and is filled with renewed energy.
In SIlicon Valley, almost every company is fighting to hire good designers and engineers. Do you find it difficult to find and retain talent?
I have this frustration that the nonprofit sector pays very talented people not very much money because they have chosen this field. We try to pay people market salaries, despite the push-back from donors. I think our employees are worth even more than what we're paying them.
Overall though, we've done well with recruiting. Where it gets challenging is with more senior staff; people with nonprofit experience and medical device experience.
Any parting words of wisdom for would-be health entrepreneurs who want to help low-income people?
Get out there and get experience. Talk to people; learn how to frame questions. Every time I go on vacation for instance, I stop into clinics and hospitals that use our products. Whenever I do field work, I always learn new things.
Sponsored
[ted id=1895]
lower waypoint
Explore tiny wildlife wonders up close with science and nature news by the award-winning Deep Look team.
To learn more about how we use your information, please read our privacy policy.