San Francisco General Hospital emergency and neurocritical care physician Debbie Yi Madhok by the hospital's emergency room CT scanner. (Beth Winegarner )
The last thing Donna Taylor remembers about the night of July 21, 2017, is her intense headache and flickering vision.
When her husband, Joseph, found her lying on the floor of their San Francisco home, she couldn’t get up, so he called 911.
“I realized this was not something we can handle here at home,” Joseph says. “This was awfully scary.”
The ambulance took Taylor, 55, to Zuckerberg San Francisco General Hospital and Trauma Center, where she was rushed to get a CT scan. The doctors found a large clot blocking one of the major arteries to her brain -- a stroke. Within 28 minutes of her arrival, Donna was given medication to break up the clot. Within 108 minutes, surgeons were removing it. By the next day, she was mobile again.
This protocol was new. It was developed by emergency and neurocritical care physician Debbie Madhok.
Sponsored
"There’s an old adage that ‘time is brain,’” says Madhok. “It’s been shown that if you occlude a big blood vessel in the brain, about 2 million brain cells die per minute. Depending on where these cells die, the impact can be quite devastating.”
People who suffer massive strokes can permanently lose the ability to speak or move parts of their bodies. For every hour that treatment is delayed, a stroke patient loses 3.6 years of functional life, says J. Claude Hemphill III, one of San Francisco General's neurosurgeons.
The American Heart Association recommends stroke patients receive the clot-busting medicine known as tPA within 45-60 minutes of arriving at a hospital. But under Madhok’s plan, treatment comes faster.
It starts with the paramedics calling ahead when transporting a potential stroke patient. They are met at the emergency room doors by a stroke specialist who moves the patient just a few yards, to be weighed and given a CT scan. If the scan reveals that a large clot is cutting off blood supply to the brain, the patient immediately receives a weight-appropriate dose of tPA while still in the scanner. Soon after, a surgical team removes the clot.
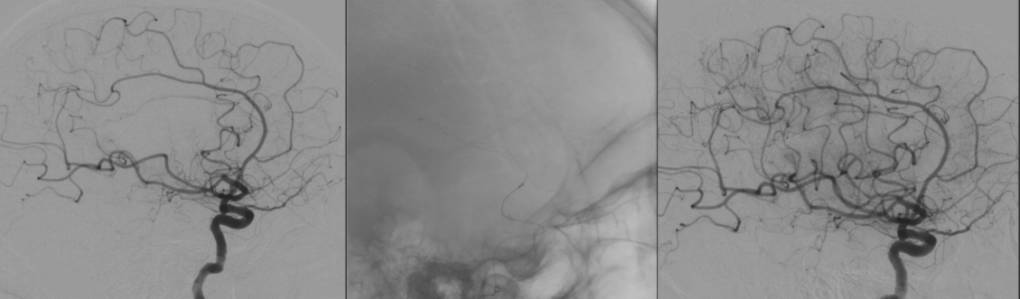
X-ray scans of the brain (a cerebral angiogram) show where a stroke patient's blood flow is blocked (left), the clot being removed (middle) and blood flow restored (right). (San Francisco General Hospital)
Madhok calls it the Mission Protocol, both because it’s her mission to streamline emergency stroke treatment and because the hospital sits on the border of San Francisco’s Mission district, providing care for many of its residents.
Under the protocol, the median time for patients to get a CT scan is 10 minutes , which is 13 minutes faster than before. The median from "door-to-needle,” the time it takes to administer tPA, is 20 minutes, less than half the 45 minutes it used to take.
Several studies have shown that mechanical thrombectomy, in which doctors snake tiny tools into a patient’s artery to remove clots, is a key step in emergency stroke care. While the Committee of the Society of Vascular and Interventional Neurology recommends clot removal in less than 90 minutes, under the Mission Protocol, the hospital’s median time to remove clots is 76 minutes.
In response to those studies, more hospitals are adding mechanical thrombectomy to their emergency stroke care, says Dr. Jose Biller, neurology chair at the Loyola University Chicago Stritch School of Medicine.
“Everyone I know of is very cognizant of the fact that early stroke treatment is essential,” Biller says. “You see variations on this theme in many institutions.”
Shaving Time to Treatment
Two initiatives in the past decade began to affect how hospitals treat stroke patients. In 2010, the American Heart Association launched Target: Stroke, an initiative aimed at encouraging hospitals to reduce their door-to-needle time to less than 60 minutes. Two years later, research out of Helsinki showed how to shave off minutes from that time, and many hospitals began adopting the method.
“It’s become a competitive thing, seeing who can go for the quickest time possible,” says David Tong, a neurologist with California Pacific Medical Center and a member of the American Neurological Association's Advisory Committee. “Over the past 10 to 15 years, that has dramatically improved. But it takes a lot of coordination.”
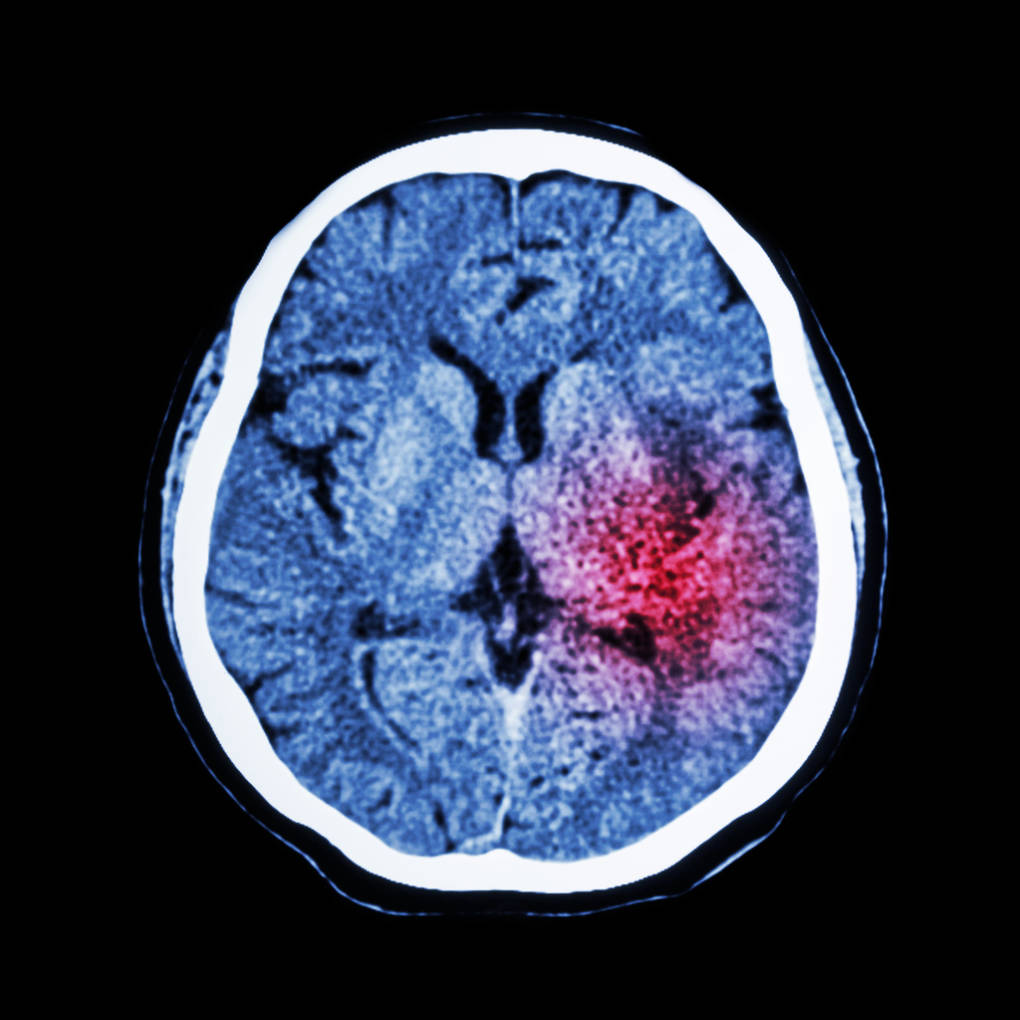
CT scan of a brain showing a stroke (iStockphoto)
One study found that hospitals participating in the AHA initiative from 2009-2013 improved their average door-to-needle time from 74 down to 59 minutes. Patients’ in-hospital deaths dropped close to 2 percent, and more patients were able to recover at home instead of a rehab facility, according to the AHA.
Tong says no regulation requires hospitals to follow the AHA’s recommendations for door-to-needle times, so there’s no way to know how many hospitals have made these changes. But the nationwide statistics aren’t encouraging; in 2017, according to the American Stroke Association, fewer than 30 percent of stroke patients received tPA within an hour of arrival.
And even an hour is still too long, say stroke experts.
“Some hospitals say a 60-minute door-to-needle time is good,” says Hemphill. “Now, when we treat someone in 60 or 45 minutes, we ask, ‘What went wrong?’ We regularly treat patients within 20 minutes.”
Closing the Gender and Race Gaps
Madhok reached out to San Francisco General to develop her protocol because the hospital provides emergency medicine to underserved populations, as well as doing neurocritical care research. The hospital wasn’t hiring, but once doctors heard what she wanted to do, they found space.
As a handful of studies show, people of color and women tend to receive inferior care when they’re having a stroke, and they are less likely to receive tPA or have their clots removed. Loyola’s Dr. Biller says that lack of awareness about stroke symptoms, or the fact that high blood pressure is a precursor to stroke, may explain some of the disparities in treatment.
“Not surprisingly, these patients also have worse short- and long-term outcomes after stroke,” Madhok says. “Organized stroke care has the potential to reduce these disparities. Mission Protocol was my way to put this to the test.”
Among the roughly 80 patients who have been subject to the protocol since July, three-quarters are Latino, Asian or black. Madhok is still gathering data for publication on long-term outcomes. Already, though, she has some idea what the results will look like.
Sponsored
“If a 20-minute delay in care can cost a patient 1.2 years of functioning brain health, then you can imagine what getting a patient to tPA in less than 20 minutes, as opposed to 45 to 60 minutes, and getting a clot open in less than 90 minutes, as opposed to two hours, means for a patient.”
lower waypoint
Explore tiny wildlife wonders up close with science and nature news by the award-winning Deep Look team.
To learn more about how we use your information, please read our privacy policy.