A pin officers wear to show they've received Crisis Intervention Training. (Alex Emslie/KQED)
San Francisco police officers Kenneth Cha and Colin Patino didn't know what they were walking into when they arrived at 515 Capitol Ave. before dawn on Jan. 6 and attempted to contact Sean Moore about a complaint from his neighbor.
The encounter with Moore escalated into the Police Department's first officer-involved shooting of 2017 and the first ever in San Francisco to be captured on police body cameras. It was also the latest example of a tragic trend in San Francisco and across the nation: People in the midst of a psychiatric crisis make up a disproportionate number of those shot by police.
It's a disparity San Francisco has struggled to reduce for over a decade. That effort involves a police practice called Crisis Intervention Training, or CIT, which teaches officers to recognize the signs of mental illness and techniques to de-escalate the heightened emotional state of someone in psychiatric distress.
The SFPD has made strides in the effort, instituting new use-of-force and CIT policies with de-escalation at their core -- and sending over 700 officers, or about half of patrol officers, through the 40-hour training. But the Moore shooting exposed a long-standing problem of identifying people in psychiatric crisis and getting that information to responding officers.
"I saw aspects of our training come through in terms of how the police handled it," said David Elliot Lewis, a civilian trainer in SFPD's CIT program and a member of the city's mental health board. "It wasn’t ideal, no. CIT is a work in progress, and there’s still work to be done."
Sponsored
The Shooting
Moore is diagnosed with bipolar disorder and schizophrenia, according to his brother and his defense attorney. He has a reputation among neighbors for hostility, but not necessarily violence. Police had helped get Moore to the hospital for emergency psychiatric treatment several times in the past, according to his mother.
Moore's neighbor, Christopher Choy, had recently filed for a restraining order in civil court, describing threats from Moore and repeated banging on a wall the two homes share in the city's Ocean View neighborhood. The complaint notes a criminal conviction against Moore in 2011 and multiple calls to police since, when officers apparently were unable to talk to Moore. The restraining order request was scheduled for a hearing on Jan. 11.
Information about Moore's psychiatric history doesn't appear to have made it to Cha and Patino, though, neither of whom are trained in crisis intervention.
When they contacted Moore, he was angry and said he was going to "call to remove you," then slammed his door.
Editors note: The following video contains profanity and violence.
Cha and Patino backed off, but Moore came back out, and they again climbed his staircase. When he opened his gate and moved toward the officers, Cha pepper-sprayed him, also hitting Patino. Moore scrambled back inside his house. Cha called for an ambulance, and when Moore came out again, both officers tried to move in to arrest him.
They fought on the narrow staircase. Patino hit Moore with his baton twice, then Moore punched the officer in the face, fracturing his nose and sending him toppling to the street. He kicked Cha, who fired twice as he fell down the stairs.
Moore was hit in the groin and abdomen. He retreated inside his house and called 911 to report he'd been shot. Police arrested him over an hour later. He was taken to the hospital and had major surgery. Moore remains in custody and faces felony assault and battery charges.
Deployment Unclear
There's little agreement on whether the incident that led to Moore's shooting should have elicited a CIT response.
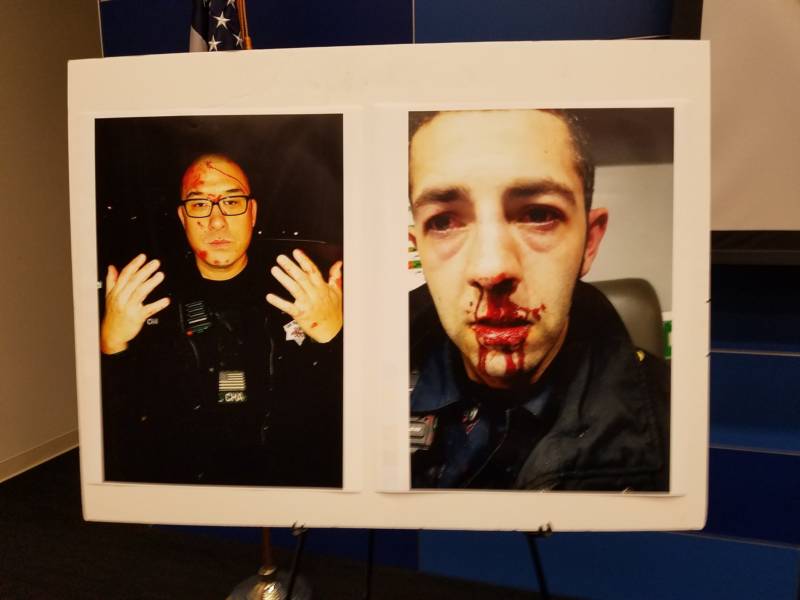
Photographs of SFPD officers Kenneth Cha and Colin Patino following their Jan. 6 encounter with Sean Moore as displayed at a Police Department press conference on Jan. 18. (Alex Emslie/KQED)
Then Acting Police Chief Toney Chaplin said in January that officers don't memorize the addresses they're called to, and Cha and Patino had no way of knowing the call about a temporary restraining order would involve mental health issues. He said the department is looking into creating a database of addresses where mental illness has been an issue in the past.
"The Police Department is trying to develop a database of people who they frequently contact who have mental health crisis issues or behavioral health issues, who have frequent contact with medical authorities and law enforcement," Lewis said. "And once this database is deployed, then when going out on a call, they’ll have more information up front that the person has a history of mental illness that might need a different approach."
But the Department of Emergency Management, which handles 911 calls and dispatch in San Francisco, already has the ability to search by name and address for past psychiatric emergencies, according to Deputy Director Rob Smuts.
"There are mechanisms to do that," he said. "What we are trying to do is make sure that the training is in place so we are consistently doing that. For years and years and years, we do that search if there is a premise record of somebody who had a gun or had a knife or something like that. We also really want to make an emphasis on any information that might inform the police’s interaction when they get there, and that’s the mental health history, and that’s not as long-standing a practice in police dispatch world."
Sean Moore (Courtesy of Kenneth Blackmon)
It's unknown whether dispatch ran a search on Moore. The Department of Emergency Management declined to provide that information, citing ongoing investigations into the shooting.
Even if the officers didn't know Moore's history, his family and attorneys say the signs were clear, and they should have backed off and waited for things to calm down.
"Instead, the officers went up the stairs and essentially escalated the situation," San Francisco Public Defender Jeff Adachi said at a press conference where he released police body-camera video of the shooting. "This is a situation that could have and should have been avoided. Mr. Moore did not have to be shot, and the officers, had they properly used de-escalation techniques, would have gone home."
Sean Moore's mother, Cleo Moore, spent 40 years as a nurse at San Francisco General Hospital, where her son was treated for gunshot wounds.
"Something has to be done not only to help the mentally ill in this city, and the Police Department needs to be changed to learn how to deal with mentally ill patients," she said outside a recent court hearing for her son. "Back off from the situation, call Crisis Intervention. The city has crisis intervention. They could have come out and helped them to diffuse the situation. Don’t shoot somebody."
San Francisco Public Defender Jeff Adachi and Deputy Public Defender Brian Pearlman release SFPD body-camera video on Jan. 18. The video captured the Jan. 6 police shooting of Sean Moore. (Alex Emslie/KQED)
SFPD Lt. Mario Molina, who heads the Police Department's Crisis Intervention Team, said he can't speak in any detail about the incident that remains under investigation. But in general, SFPD's push to train every officer in CIT encourages officers to collect more information.
"The effort is for officers to start thinking the minute they get the call," he said. "Start asking questions, gather more information. And evaluate, reassess, reassess. We continue to emphasize that. Reassess the situation. What do you have? What are you dealing with? What resources will you need?"
Lewis said even if Moore's psychiatric history was unclear, the need for de-escalation tactics was obvious.
"Being that angry and that triggered and that escalated clearly is a mental health issue," he said. "Maybe it doesn’t need to have a diagnostic label, but it does call for de-escalation because somebody that angry isn’t listening."
Crisis Calls Undercounted
Dispatch data show a significant undercount in police incidents involving mental illness. The Department of Emergency Management started cataloging police calls that should get a specialized crisis response in May 2014, according to data provided by the department. Since then, 932 "CR" codes have been appended to police incidents, an average of about one per day.
"We average about 13,000 every three months," said Molina. That includes attempted suicides, people in general mental distress, children beyond the control of their parents, well-being checks and requests for involuntary mental health detentions, known by the legal code 5150. Molina said officers were dispatched and made contact in a smaller set of those calls, but still averaging at least 30 per day.
"When you told me one a day, that's way under-reported," he said. "Cops are going to calls after calls. I've been there. I've done it, and we're dealing with this on a daily basis."
The vast majority of the time, those calls end peacefully. When they don't, there's a disproportionate amount of focus, Molina said.
"I don’t want to sound defensive here, but you also have to give the benefit to the officer," he said. "You had the benefit to have a video recorder apparatus and then you were able to see it 20,000 times later on, and that officer had one second, or a half a second to make that decision. And they did it because they felt like their life was in danger, or somebody else’s life was in danger."
There's a new round of changes coming to the Police Department's crisis intervention effort, though, ones that will alter the way teams of four officers with the training are deployed. Molina is also hopeful that police will get some help from city psychologists to prevent psychiatric crises from happening in the first place.
Changes Coming
SFPD is rolling out a 20-hour tactical training for officers on the department's new use-of-force rules. Lewis said it will augment the role-playing segments of crisis intervention training, which never lead to a physical struggle.
He said the body-camera footage from the Moore shooting could be useful in the training.
"That was a highly volatile encounter, and one that we haven’t been training to but we will be training to," Lewis said.
The "crisis response" police code is also changing, according to Smuts and Molina, to become a signal to deploy a team of officers prepared to confront a mentally ill suspect with a weapon other than a gun.
The approach involves teams of four officers in different roles, all assigned at the beginning of the week so it's in place when a crisis begins.
The contact officer will talk to the suspect while covered by two other officers, one likely armed with a beanbag shotgun or other "less lethal" weapon, and the other with a firearm. The fourth officer will keep an eye on any bystanders and reach out to people who may have knowledge of the suspect.
There's also a yet-to-launch pilot program that will link five city mental health clinicians with the Police Department.
The city's Department of Public Health envisions that, with some fill-ins, at least one psychologist or social worker will be available 24 hours a day to consult with police while officers attempt to contact suspects in psychiatric crisis. The clinicians will not make direct contact with people in crisis.
"Our goal is really to support police officers in de-escalating these situations," said Angelica Almeida, director of assisted outpatient treatment at DPH. "They'll also be able to provide that ongoing support because, beyond a critical incident, we want to make sure that we are preventing any future incidents that are happening. So we want to be able to plug individuals into our already robust system of care that they may not otherwise have tapped into."
To Molina, making those connections is a huge priority.
Sponsored
"I want to be proactive," he said. "I don't want the crisis."
lower waypoint
Stay in touch. Sign up for our daily newsletter.
To learn more about how we use your information, please read our privacy policy.